Introduction

Bacterial endotoxin testing is one of the most critical quality control procedures in the pharmaceutical, biotechnology, medical device, and cell therapy industries. Whether testing injectable drugs, biologics, vaccines, medical devices, or laboratory reagents, laboratories must ensure that endotoxin levels comply with regulatory requirements before products are released.
Among the compendial methods described in USP <85>, EP 2.6.14, JP, and ChP, two techniques are widely adopted:
Both methods rely on the same biological principle—the enzymatic coagulation cascade of horseshoe crab amoebocyte lysate (TAL/LAL)—yet they differ significantly in workflow, throughput, data output, equipment requirements, and overall cost.
Many laboratories ask the same questions before purchasing an endotoxin test kit:
- Is the Gel Clot method still suitable for modern laboratories?
- Is a Kinetic Chromogenic assay worth the investment?
- Why do Gel Clot assays fail even when the reagent appears to be fine?
- How can recurring failures be prevented?
This guide answers these questions with practical recommendations based on laboratory workflows rather than marketing claims.
Understanding the Two Methods
Gel Clot Method
The Gel Clot assay is the oldest and simplest bacterial endotoxin testing method and remains the reference limit test recognized by all major pharmacopoeias.
The assay is based on a simple principle:
When endotoxin is present, it activates the enzyme cascade within the TAL/LAL reagent, ultimately producing an insoluble coagulin gel.
After incubation at 37 ± 1°C for 60 ± 2 minutes, the reaction tube is gently inverted.
- An intact clot remains in place: Positive.
- The clot collapses or flows: Negative.
Because the endpoint is determined visually, no microplate reader or specialized software is required.
Advantages
- Lowest equipment cost
- Simple workflow
- Pharmacopoeia accepted worldwide
- Excellent for endotoxin limit testing
- Suitable for laboratories with low testing volumes
Limitations
- Qualitative only
- Manual interpretation
- Low throughput
- Higher operator dependence
- Difficult to automate
Kinetic Chromogenic Method
The Kinetic Chromogenic assay uses the same TAL/LAL enzyme cascade but measures endotoxin quantitatively.
Instead of observing clot formation, the activated enzyme cleaves a synthetic chromogenic substrate, producing a yellow color that increases over time.
A compatible microplate reader continuously measures absorbance at 405 nm, and dedicated software automatically calculates:
- Standard curve
- Endotoxin concentration
- Correlation coefficient
- Spike recovery
- Coefficient of variation (CV)
The result is objective, quantitative, and fully traceable.
Advantages
- Quantitative results
- High throughput
- Excellent reproducibility
- Automated calculations
- Electronic data management
- Lower labor cost for routine testing
Limitations
- Requires a compatible microplate reader
- Higher initial equipment investment
- More comprehensive operator training
Gel Clot vs. Kinetic Chromogenic: A Side-by-Side Comparison
| Feature | Gel Clot | Kinetic Chromogenic |
|---|---|---|
| Result | Qualitative | Quantitative |
| Detection | Visual | Spectrophotometric |
| Equipment | Incubator only | Microplate reader |
| Data recording | Manual | Automatic |
| Throughput | Low | High |
| Automation | None | Excellent |
| Initial investment | Low | Moderate |
| Cost per sample | Higher at large volumes | Lower at large volumes |
| GMP data traceability | Limited | Excellent |
Which Method Is Right for Your Laboratory?
The answer depends on testing volume, regulatory requirements, available equipment, and long-term operating costs.
Gel Clot is the Better Choice If You:
- Test only a few samples each week.
- Need a simple pass/fail result.
- Have limited laboratory equipment.
- Prefer the lowest initial investment.
- Perform routine endotoxin limit testing.
Kinetic Chromogenic is the Better Choice If You:
- Process dozens of samples every day.
- Require quantitative endotoxin values.
- Need electronic records for GMP compliance.
- Want to reduce labor costs.
- Need high-throughput testing.
Why Looking Only at Kit Price Can Be Misleading
Many purchasing decisions focus solely on the price of the endotoxin reagent kit.
However, the total cost of testing includes much more than reagent cost.
For example, a Gel Clot assay requires manual preparation, individual reaction tubes, visual interpretation, and more technician time. As testing volume increases, labor becomes a major contributor to the overall cost.
In contrast, a Kinetic Chromogenic assay uses a 96-well microplate. Once the plate is prepared, dozens of samples can be analyzed simultaneously, dramatically reducing labor and the average cost per sample.
Example:
A standard 96-well kinetic chromogenic assay can typically analyze:
- Up to 43 samples when using duplicate measurements with a standard curve and negative controls.
- Approximately 21 samples when Positive Product Controls (PPCs) are included for every sample.
For laboratories processing routine batches, this higher throughput often outweighs the initial equipment investment.
Why Do Gel Clot Tests Fail? The Seven Most Common Root Causes
When a Gel Clot assay fails, laboratories often assume the reagent is defective. In reality, most failures are caused by issues in storage, handling, testing conditions, or laboratory technique.
Understanding these root causes can help reduce repeat testing, save time, and improve confidence in the results.
1. Improper Storage and Transportation
The TAL/LAL reagent contains temperature-sensitive enzymes.
Common problems include:
- Exposure to elevated temperatures during shipping.
- Storage outside the recommended temperature range.
- Multiple freeze–thaw cycles.
- Using expired reagents.
How to Prevent It
- Follow the manufacturer's storage instructions.
- Minimize the time reagents remain at room temperature.
- Avoid repeated freeze–thaw cycles.
- Monitor cold-chain transportation whenever possible.
2. Incorrect Reconstitution
Improper mixing can reduce enzyme activity.
Common mistakes include:
- Vortexing the reagent vigorously.
- Creating excessive bubbles.
- Using non-endotoxin-free water.
- Allowing the reagent to stand too long before use.
Best Practice
Reconstitute the reagent gently using certified endotoxin-free water and swirl slowly until completely dissolved.
3. Pipetting Errors
Small volume errors can produce significant differences near the assay detection limit.
Potential causes include:
- Poor pipette calibration.
- Air bubbles.
- Inconsistent pipetting.
- Incorrect sample volume.
Best Practice
- Calibrate pipettes regularly.
- Use pyrogen-free tips.
- Change tips between samples.
- Train operators on consistent pipetting techniques.
4. Incubation Problems
Gel Clot assays require strict temperature and timing control.
Common issues include:
- Incubator temperature fluctuations.
- Uneven heat distribution.
- Frequent opening of the incubator.
- Incorrect incubation time.
Best Practice
Validate the incubator regularly and avoid disturbing the assay during incubation.
5. Sample Interference
Certain formulations interfere with the TAL/LAL reaction.
Examples include:
- Extreme pH.
- High salt concentrations.
- Proteins.
- Surfactants.
- Chelating agents.
- Organic solvents.
These components may inhibit or enhance the reaction, leading to false results.
Best Practice
Always perform inhibition/enhancement studies and include PPCs during method validation.
6. Poor Interpretation of Gel Formation
Although Gel Clot appears simple, result interpretation requires experience.
Common mistakes include:
- Shaking the tube before reading.
- Rotating the tube repeatedly.
- Waiting too long before reading.
- Interpreting weak gels inconsistently.
Best Practice
Follow pharmacopoeial guidance and ensure all analysts are trained using the same interpretation criteria.
7. Environmental Contamination
Unexpected positive results may originate from contaminated consumables or laboratory environments.
Possible sources include:
- Non-pyrogen-free tubes.
- Pipette tips.
- Water.
- Airborne contamination.
- Gloves contacting sterile surfaces.
Best Practice
Use certified endotoxin-free consumables and maintain a clean working environment throughout the assay.
A Practical Troubleshooting Workflow
When a Gel Clot assay produces unexpected results, avoid immediately repeating the test without identifying the cause.
Instead, follow this sequence:
Step 1: Review Positive and Negative Controls.
↓
Step 2: Confirm reagent storage conditions.
↓
Step 3: Verify reconstitution and pipetting procedures.
↓
Step 4: Check incubator temperature and timing.
↓
Step 5: Evaluate potential sample interference.
↓
Step 6: Review operator technique and result interpretation.
↓
Step 7: Repeat the assay only after correcting any identified issues.
This systematic approach helps reduce repeat failures and improves confidence in the final result.
Preventive Best Practices for Reliable Gel Clot Testing
Successful endotoxin testing depends on consistency. The following practices can significantly reduce assay failures:
- Store reagents according to the manufacturer's recommendations.
- Use only certified endotoxin-free water and consumables.
- Calibrate pipettes and incubators on a regular schedule.
- Prepare fresh standards and controls for every assay.
- Minimize vibration during incubation.
- Include appropriate Positive and Negative Controls in every run.
- Perform routine operator training and competency assessments.
- Investigate and document all deviations from standard operating procedures.
Implementing these measures not only improves assay reliability but also supports regulatory compliance and audit readiness.
When Should You Upgrade to Kinetic Chromogenic?
Many laboratories begin with Gel Clot because it is simple and economical. However, as testing demand grows, manual workflows can become inefficient.
You should consider transitioning to a Kinetic Chromogenic assay if:
- Sample throughput continues to increase.
- Repeat testing consumes excessive technician time.
- Quantitative endotoxin values are required.
- Electronic records are needed for GMP compliance.
- Labor costs become a significant portion of testing expenses.
Many quality control laboratories successfully use both methods: Gel Clot for routine limit tests or backup confirmation, and Kinetic Chromogenic assays for high-throughput product release testing.
Gel Clot vs. Kinetic Chromogenic: A Practical Comparison
| Laboratory Scenario | Recommended Method |
|---|---|
| Startup QC Lab | Gel Clot |
| Academic Research | Gel Clot |
| Routine Pharmaceutical QC | Kinetic Chromogenic |
| Contract Testing Lab | Kinetic Chromogenic |
| High-throughput Release Testing | Kinetic Chromogenic |
The Three Most Common Causes of Gel Clot Test Failure
After reviewing feedback from customer laboratories, we have found that most Gel Clot assay failures are not caused by defective reagents. Instead, they are usually associated with deviations from the recommended operating procedure.
Among the cases we have investigated, three procedural issues account for the majority of unsuccessful Gel Clot assays.
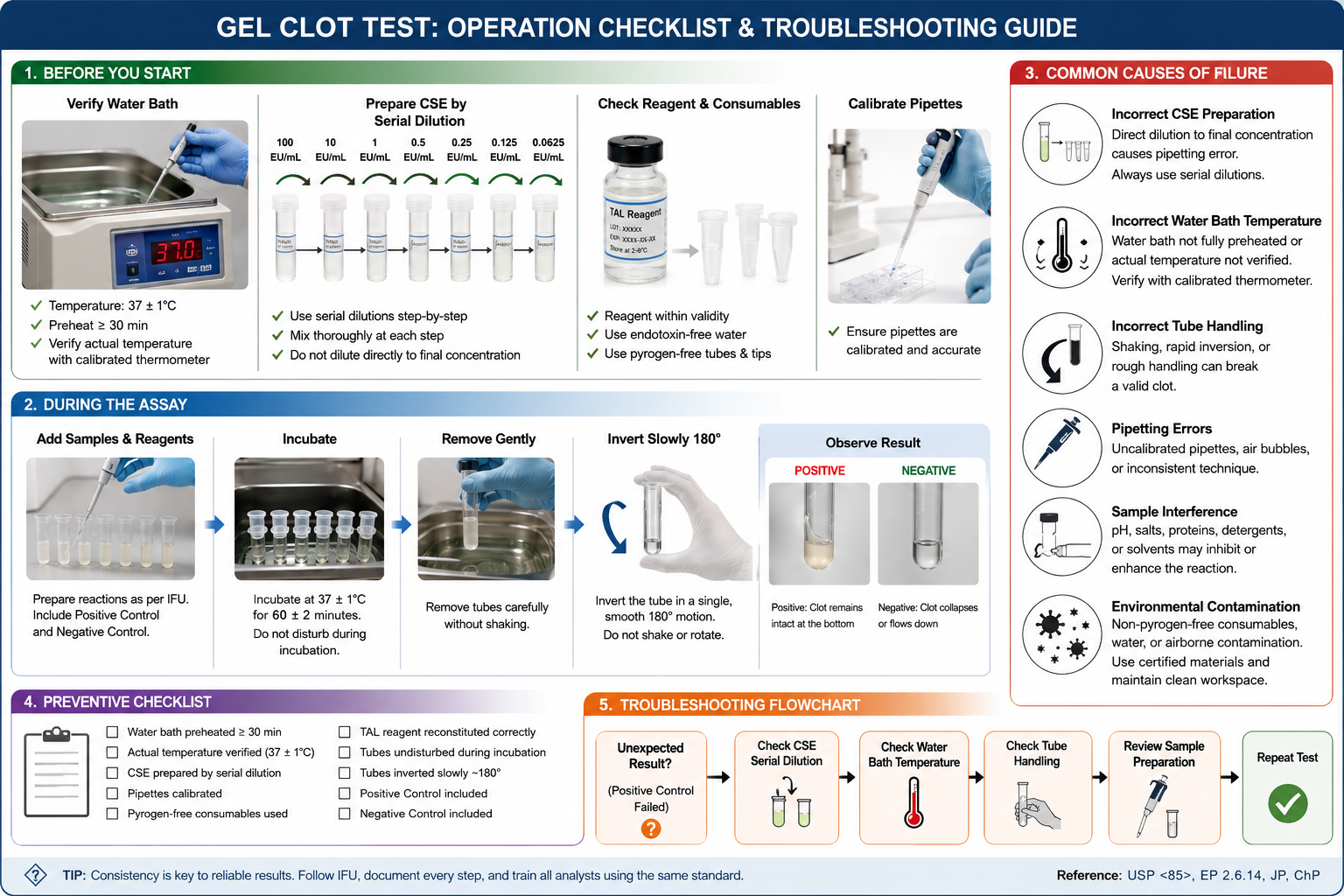
1. Incorrect Preparation of the Control Standard Endotoxin (CSE)
This is the most common issue we encounter during technical support.
When preparing the Control Standard Endotoxin (CSE), some operators dilute the stock solution directly to the final target concentration in a single step.
For example:
❌
100 EU/mL
↓
0.0625 EU/mL
Instead of following the recommended serial dilution procedure.
According to the Instructions for Use, the CSE should be prepared using stepwise serial dilutions, for example:
100 EU/mL
↓
10 EU/mL
↓
1 EU/mL
↓
0.5 EU/mL
↓
0.25 EU/mL
↓
0.125 EU/mL
↓
0.0625 EU/mL
Each dilution step should be mixed thoroughly before preparing the next dilution. This approach minimizes dilution error and helps maintain the accuracy of the positive control.
Why is this important?
A direct large-volume dilution can introduce significant pipetting error, especially when working with very low endotoxin concentrations.
This may result in:
- Weak positive controls
- Inconsistent clot formation
- Reduced assay sensitivity
- False-negative results
Best Practice
✔ Always prepare the CSE using serial dilutions as described in the Instructions for Use.
✔ Mix thoroughly after each dilution step.
✔ Use calibrated pipettes and endotoxin-free consumables.
Why does this happen?
Many analysts assume that because endotoxin concentrations are extremely low, a direct dilution will save time.
Unfortunately, this is exactly where pipetting error becomes magnified.
Real Customer Case
One customer repeatedly reported that the positive control failed during the Gel Clot assay. After reviewing the testing procedure, we discovered that the Control Standard Endotoxin had been diluted directly from the stock solution to the final concentration. Once the customer switched to the recommended serial dilution procedure described in the Instructions for Use, the positive control passed without replacing the reagent.
2. The Water Bath Was Not Fully Preheated or the Actual Temperature Was Incorrect
The Gel Clot assay requires incubation at:
37 ± 1°C for 60 ± 2 minutes
Although many laboratories set the water bath to 37°C, the displayed temperature does not always represent the actual temperature of the water.
Common issues include:
- Starting the assay before the water bath reaches equilibrium.
- Assuming the displayed temperature is accurate without verification.
- Poor temperature uniformity within the water bath.
- Lack of routine calibration.
Even a small temperature deviation may affect the activity of the TAL/LAL enzyme cascade and weaken clot formation.
Why does this happen?
Many laboratories begin testing as soon as the water bath display reads 37°C.
However, the displayed temperature may not represent the actual water temperature, especially immediately after startup.
Water also requires time to reach thermal equilibrium.
Technical Tip
We recommend preheating the water bath for at least 30 minutes before testing and verifying the actual temperature with an independent calibrated thermometer.
Best Practice
✔ Turn on the water bath well in advance of testing.
✔ Confirm the actual water temperature using a calibrated thermometer before incubation.
✔ Perform routine temperature verification and maintenance.
✔ Avoid opening the water bath frequently during incubation.
3. Incorrect Tube Handling After Incubation
This issue is often underestimated but can easily lead to weak positive or false-negative results.
After incubation, the clot formed by the Gel Clot assay—especially near the sensitivity limit—may still be delicate.
Some operators remove the tube quickly, shake it, or invert it abruptly.
These actions can break a valid clot before it is evaluated.
Correct Procedure
After the 60-minute incubation:
- Carefully remove the tube from the water bath or dry block.
- Hold the tube upright without shaking.
- Slowly invert the tube approximately 180° in one smooth motion.
- Observe whether the clot remains intact.
The tube should not be shaken, rotated repeatedly, or inverted abruptly.
Why does this matter?
A weak but valid clot may collapse if the tube is handled too aggressively, leading to:
- Weak positive reactions
- False-negative interpretations
- Unnecessary repeat testing
Best Practice
✔ Remove each tube gently.
✔ Invert the tube only once using a slow, controlled 180° motion.
✔ Ensure all analysts are trained to interpret clot formation consistently.
A Simple Troubleshooting Flowchart
Positive Control Failed?
│
▼
Check CSE Serial Dilution
│
▼
Check Water Bath Temperature
│
▼
Check Tube Handling
│
▼
Review Sample Preparation
│
▼
Repeat Test
Preventive Checklist Before Every Gel Clot Test
Before starting each assay, confirm the following:
☑ Water bath has reached 37 ± 1°C.
☑ Actual temperature verified.
☑ CSE prepared by serial dilution.
☑ Pipettes calibrated.
☑ Pyrogen-free consumables used.
☑ TAL reagent reconstituted correctly.
☑ Tubes remain undisturbed during incubation.
☑ Tubes inverted slowly by approximately 180°.
☑ Positive Control included.
☑ Negative Control included.
Frequently Asked Questions
Is the Gel Clot method less accurate than the Kinetic Chromogenic method?
Not necessarily. When performed correctly, both methods are compendial and reliable. The key difference is that Gel Clot provides a qualitative pass/fail result, whereas Kinetic Chromogenic delivers quantitative endotoxin concentrations.
Why does my Positive Product Control (PPC) fail?
A failed PPC often indicates product interference rather than reagent failure. Inhibitory or enhancing substances in the sample matrix should be investigated through inhibition/enhancement testing.
Can I switch from Gel Clot to Kinetic Chromogenic without revalidation?
Method changes typically require validation according to applicable pharmacopeial and regulatory guidelines. Consult your internal quality procedures before implementing a new assay.
Which method is more economical?
For laboratories with low testing volumes, Gel Clot usually offers the lowest upfront cost. For routine testing of larger batches, Kinetic Chromogenic assays generally provide a lower overall cost per sample because of their higher throughput and reduced manual labor.
Conclusion
Both Gel Clot and Kinetic Chromogenic assays remain indispensable tools for bacterial endotoxin testing. Rather than asking which method is "better," laboratories should evaluate which method best aligns with their workflow, sample volume, regulatory requirements, and long-term operating costs.
For laboratories with limited testing needs, the Gel Clot method continues to provide a simple, reliable, and pharmacopoeia-compliant solution. For laboratories seeking greater efficiency, quantitative results, and lower cost per sample, Kinetic Chromogenic assays offer clear operational advantages.
By understanding the strengths, limitations, and common failure modes of each method—and by implementing robust preventive practices—quality control laboratories can improve testing reliability, reduce repeat analyses, and maintain confidence in endotoxin test results.
FireGene Endotoxin Testing
Ready to run your endotoxin assay?
FireGene offers a complete endotoxin testing toolkit — from TAL reagents and CSE standards to pyrogen-free consumables and LAL reagent water. All products are aligned with USP <85>, EP 2.6.14, and JP 4.01.





